Abstract
- A 29-year-old patient with diplopia showed a unilateral fourth nerve palsy combined with a Horner syndrome on the opposite side. Magnetic resonance images disclosed a focal hemorrhage in the left dorsal midbrain, affecting the nucleus of the fourth nerve and adjacent oculosympathetic fibers. Further evaluations including a bone marrow biopsy confirmed acute lymphoblastic leukemia. The combination of ocular motor and oculosympathetic palsy has a distinct localizing value. Fourth nerve palsy ipsilateral to Horner syndrome locates lesion in the cavernous sinus, while contralateral fourth nerve palsy locates the lesion in the midbrain.
-
Keywords: Diplopia; Horner syndrome; Trochlear nerve; Hemorrhage; Leukemia
-
중심단어: 복시, 호너 증후군, 활차 신경, 백혈병
INTRODUCTION
While peripheral fourth nerve palsies are commonly caused by trauma or ischemia, central fourth nerve palsy from a lesion in the brainstem is uncommon [1-3]. Although rare, the combination of superior oblique palsy and contralateral brainstem signs, especially Horner syndrome or cerebellar ataxia, has a localizing value [4]. This study describes a patient with acute leukemia which was presented as contralesional fourth nerve palsies and ipsilesional Horner syndrome from an intraaxial lesion within the dorsal midbrain.
CASE REPORT
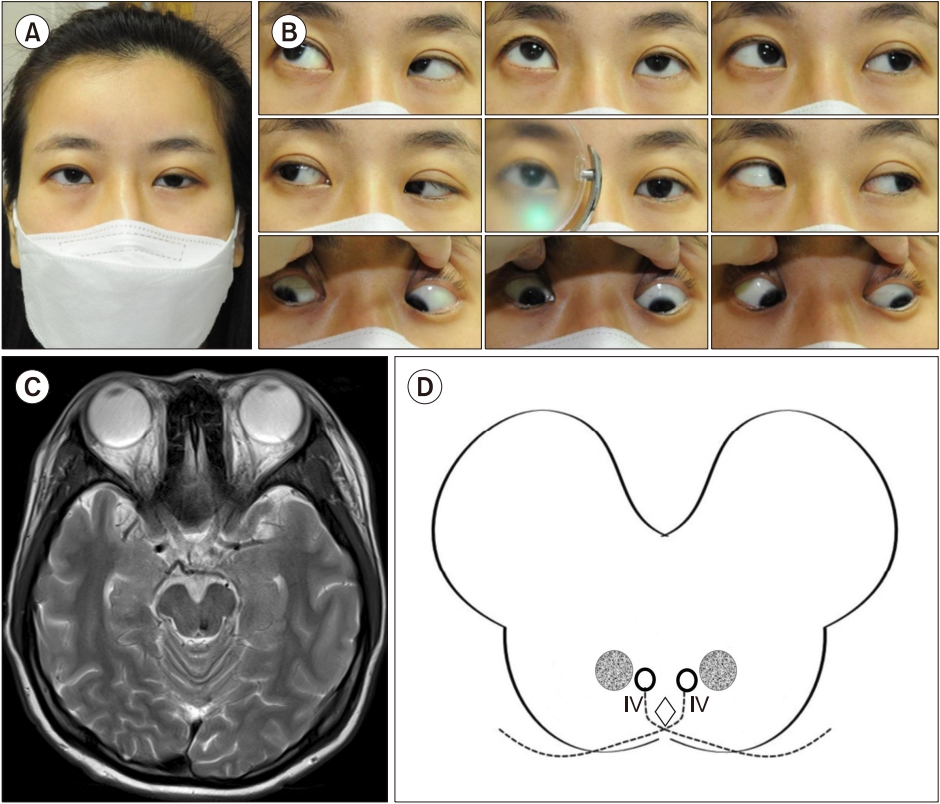
A 29-year-old woman without a medical history presented with 6 days of binocular vertical diplopia and a left eyelid droop. She also had noted sudden headache and general weakness. She showed leftward tilted head position, left-sided ptosis and miosis (Fig. 1A). The eyelids exhibited no daily variations, and the icepack test was negative. In the neutral position, she showed hypertropia of the right eye (7 prism diopter), which worsened during leftward gaze (9 prism diopter), downward gaze (18 prism diopter), and rightward head tilt (25 prism diopter) (Fig. 1B). Other neurologic findings including limb ataxia, facial sweating, and hearing were normal. Fundus photography did not show abnormal ocular torsion. Brain computed tomography and magnetic resonance imaging revealed a focal hemorrhagic lesion within the left dorsal midbrain tegmentum (Fig. 1C). Cerebrospinal fluid analysis showed elevated red blood cells (180/mm3) and other contents were normal. Analysis of blood contents showed severe leukocytosis (white blood cells, 652,270/mm3), anemia (hemoglobins, 8.5 g/dL), and thrombocytopenia (platelets, 20,000/mm3). Further evaluations including a bone marrow biopsy confirmed acute lymphoblastic leukemia. With the management of leukemia, both the Horner syndrome and the fourth nerve palsy resolved 2 months later.
Written informed consent was obtained for publication of this case report and accompanying images.
DISCUSSION
The present case showed an unusual combination of trochlear nerve palsy and crossed Horner syndrome from a brainstem hemorrhage that was attributed to acute leukemia-related coagulopathy. The fourth nerve is the only nerve that arises from the dorsal aspect of the brainstem, and all of its fibers cross the midline within the brain parenchyma [5]. Lesions of the trochlear nerve cause vertical or oblique diplopia by impairing the ability of the superior oblique muscle to intort and depress the eye. While skew deviation, vertical strabismus caused by a supranuclear brainstem lesion, is not usually affected by gaze direction, the vertical diplopia from a trochlear lesion worsens in downgaze, lateral gaze away from the affected eye, and upon head tilt toward the affected eye, as seen in the present case.
The fourth nerve nucleus is located within the midbrain adjacent to periaqueductal gray matter and dorsal to the medial longitudinal fasciculus at the level of the inferior colliculus [1,5]. After leaving the nucleus, the fascicles of the fourth nerve decussate in the anterior medullary velum at the roof of the aqueduct of Sylvius and then exit the brainstem dorsally (Fig 1D). Thus, a lesion of the fourth nerve nucleus results in a superior oblique palsy of the contralateral eye. In addition, the proximity of the left fourth nerve nucleus to the descending oculosympathetic pathways resulted in the combination of a contralesional (right) superior oblique palsy with an ipsilesional (left) Horner syndrome, as shown in the present case. Lesions of the fourth nerve nuclei or fascicles should be suspected whenever a fourth nerve palsy is accompanied by brainstem signs including Horner syndrome, and the location of the lesion should be presumed to lie within the dorsal midbrain contralateral to the affected eye.
Because the oculosympathetic pathway does not decussate, damage to the unilateral oculosympathetic pathway anywhere along its course results in an ipsilesional Horner syndrome [6]. As the oculosympathetic pathway is quite long, a wide range of neurological, tumoral, and vascular lesions can produce Horner syndrome. Lesions of the hypothalamus can cause an ipsilateral Horner syndrome with contralateral hemiparesis and contralateral hypesthesia [7]. Lesions of the thalamus result in contralateral ataxic hemiparesis, contralateral hypesthesia, vertical gaze paresis, and dysphasia. The combination of a unilateral Horner syndrome and a contralateral trochlear nerve paresis, as shown in our case, suggests a lesion of the dorsal mesencephalon. Combined fourth nerve paresis and ipsilateral Horner syndrome have previously been reported in a patient with a meningioma of the lateral wall of the cavernous sinus [8]. Pontine lesions can produce a Horner syndrome associated with an ipsilateral abducens nerve paresis, and lateral medullary infarction produces a central Horner syndrome along with various neurologic signs consisting of Wallenberg syndrome.
ARTICLE INFORMATION
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING/SUPPORT
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization, Data curation, Project administration: SHK; Formal analysis, Investigation, Methodology: SK; Writing–original draft: SHK; Writing–review & editing: SK.
All authors read and approved the final manuscript.
Fig. 1.A 29-year-old woman presents leftward tilted head position and left-sided ptosis. (A) She shows hypertropia of the right eye, which worsens during leftward and downward gaze. (B) Axial T2-weighted images show a hemorrhagic lesion in the left caudal midbrain. (C) The fourth nerve nucleus (IV) is located within the midbrain at the level of the inferior colliculus. (D) Since the fascicles of the fourth nerve decussate in the anterior medullary velum, the patient shows contralesional trochlear nerve paresis, along with ipsilesional Horner syndrome due to involvement of the adjacent oculosympathetic tract/reticular formation (gray circle).
REFERENCES
- 1. Jeong SH, Kim SH, Lee SH, Park SH, Kim HJ, Kim JS. Central trochlear palsy: report of two patients with ipsilesional palsy and review of the literature. J Neuroophthalmol 2016;36:377–82.ArticlePubMed
- 2. Lee SU, Choi JY, Kim HJ, Kim JS. Central trochlear palsy as an isolated finding with metastatic tumor. J Clin Neurol 2018;14:254–6.ArticlePubMedPMCPDF
- 3. Chen WC, Li YS, Huang P. Isolated trochlear palsy as the only presentation of midbrain infarction: a case report. J Int Med Res 2021;49:3000605211008292. ArticlePubMedPMCPDF
- 4. Guy J, Day AL, Mickle JP, Schatz NJ. Contralateral trochlear nerve paresis and ipsilateral Horner’s syndrome. Am J Ophthalmol 1989;107:73–6.ArticlePubMed
- 5. Gold DR, Shin RK, Galetta S. Pearls and oy-sters: central fourth nerve palsies. Neurology 2012;79:e193–6.ArticlePubMed
- 6. González Martín-Moro J, Gilo Arrojo F, Rodríguez Del Valle JM, Sales Sanz A, González-López JJ, Pilo de la Fuente B, et al. Fourth nerve palsy plus contralateral Horner syndrome secondary to mesencephalic haemorrhage: an unusual crossed syndrome. Clin Exp Optom 2015;98:571–3.ArticlePubMed
- 7. Kanagalingam S, Miller NR. Horner syndrome: clinical perspectives. Eye Brain 2015;7:35–46.PubMedPMC
- 8. Ebner R. Fourth nerve paresis and ipsilateral Horner’s syndrome: an unusual association. Neuroophthalmology 2019;43:289–90.ArticlePubMedPMC
Citations
Citations to this article as recorded by




 PubReader
PubReader ePub Link
ePub Link Cite
Cite

