
Articles
- Page Path
- HOME > Res Vestib Sci > Volume 17(3); 2018 > Article
-
Case Report
뇌수막염이 동반된 Cogan 증후군 -
김형근1, 오은혜1, 정나연1, 최재환1,2

- Cogan Syndrome Accompanied with Meningitis
-
Hyung-Keun Kim1, Eun Hye Oh1, Na-Yeon Jung1, Jae-Hwan Choi1,2
-
Research in Vestibular Science 2018;17(3):119-123.
DOI: https://doi.org/10.21790/rvs.2018.17.3.119
Published online: September 18, 2018
1Department of Neurology, Pusan National University Yangsan Hospital, Yangsan, Korea
2Department of Neurology, Pusan National University School of Medicine, Yangsan, Korea
- Corresponding Author: Jae-Hwan Choi Department of Neurology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, 20 Geumo-ro, Mulgeum-eup, Yangsan 50612, Korea Tel: +82-55-360-2122 Fax: +82-55-360-2152 E-mail: rachelbolan@hanmail.net
• Received: July 17, 2018 • Revised: August 9, 2018 • Accepted: August 17, 2018
Copyright © 2018 by The Korean Balance Society. All rights reserved.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 5,094 Views
- 116 Download
Abstract
- Cogan syndrome is a rare inflammatory disease characterized by intraocular inflammation and vestibulo-auditory dysfunction. The exact etiology of Cogan syndrome is still unknown, but is currently thought to be an autoimmune disease. Cogan syndrome can be accompanied with various conditions including fever, arthritis, skin rash, aortitis, central or peripheral nerve system involvement, lymphadenopathy, splenomegaly and diarrhea. We report a case of Cogan syndrome accompanied with meningitis.
서 론
증 례
고 찰
Acknowledgments
Fig. 1.(A) Pure tone audiometry (PTA) shows bilateral sensorineural hearing loss at first admission. (B) After 6 months from symptom onset, follow-up PTA shows an improvement.
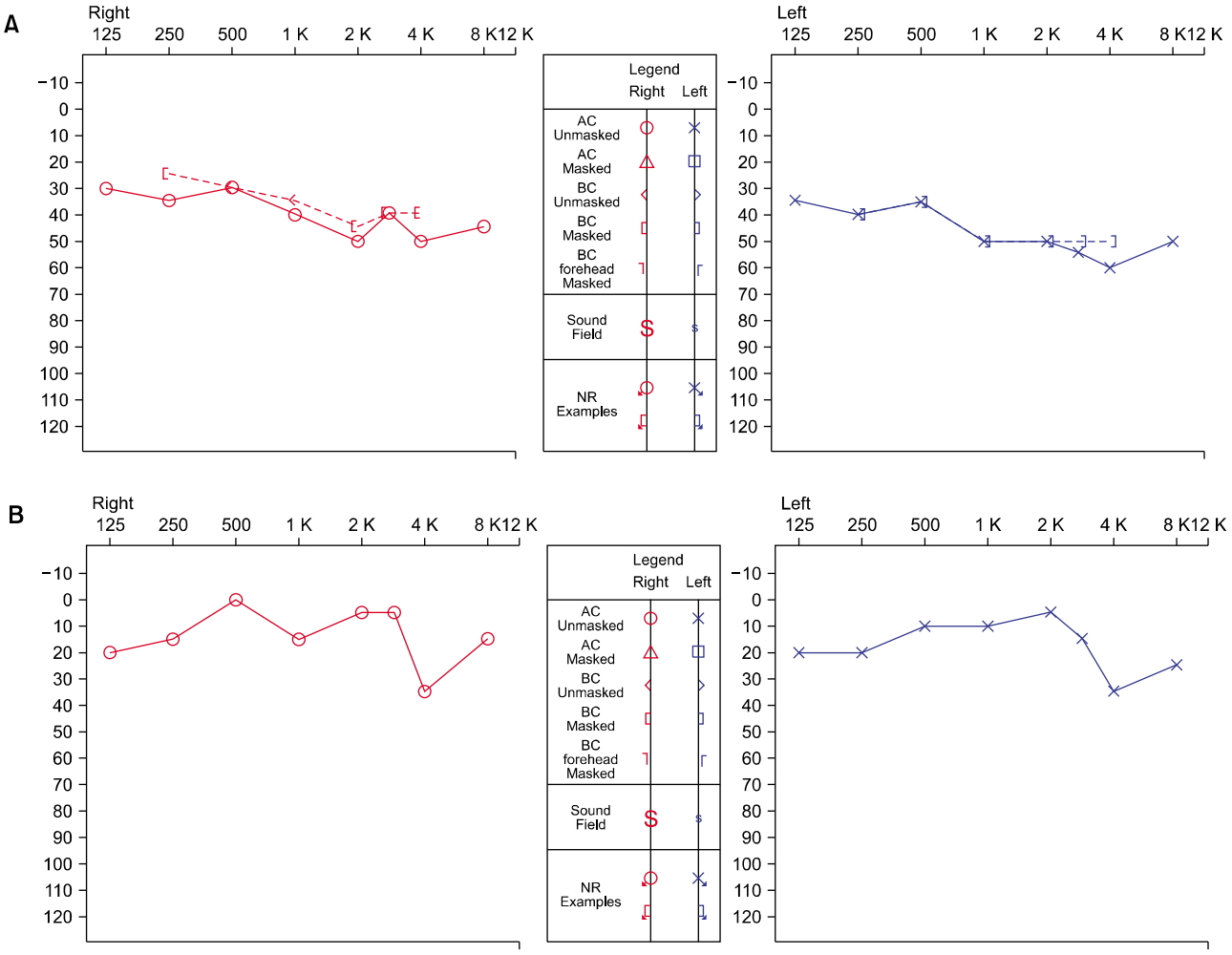
Fig. 2.Axial T1-weighted contrast enhanced magnetic resonance imaging exhibits meningeal enhancements in posterior cranial fossa and basal cistern.
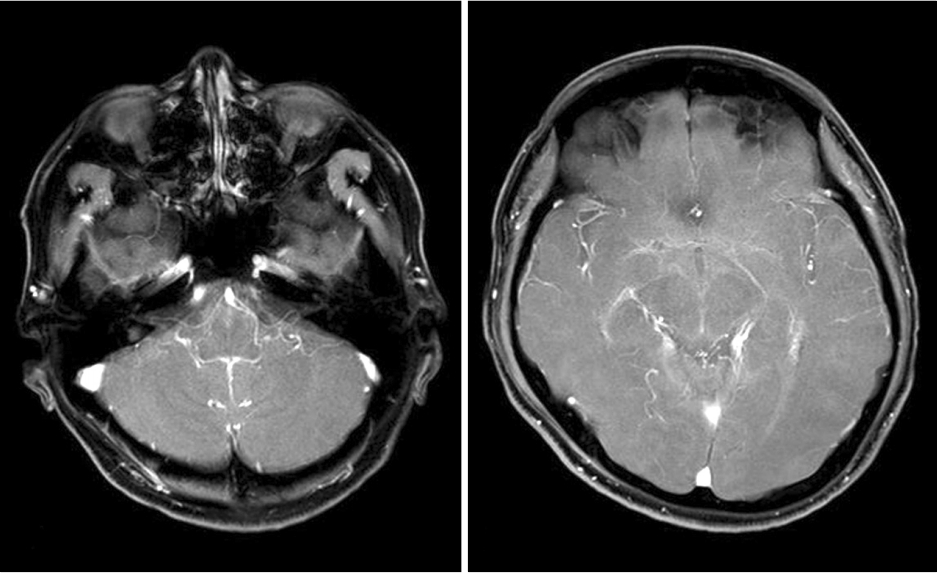
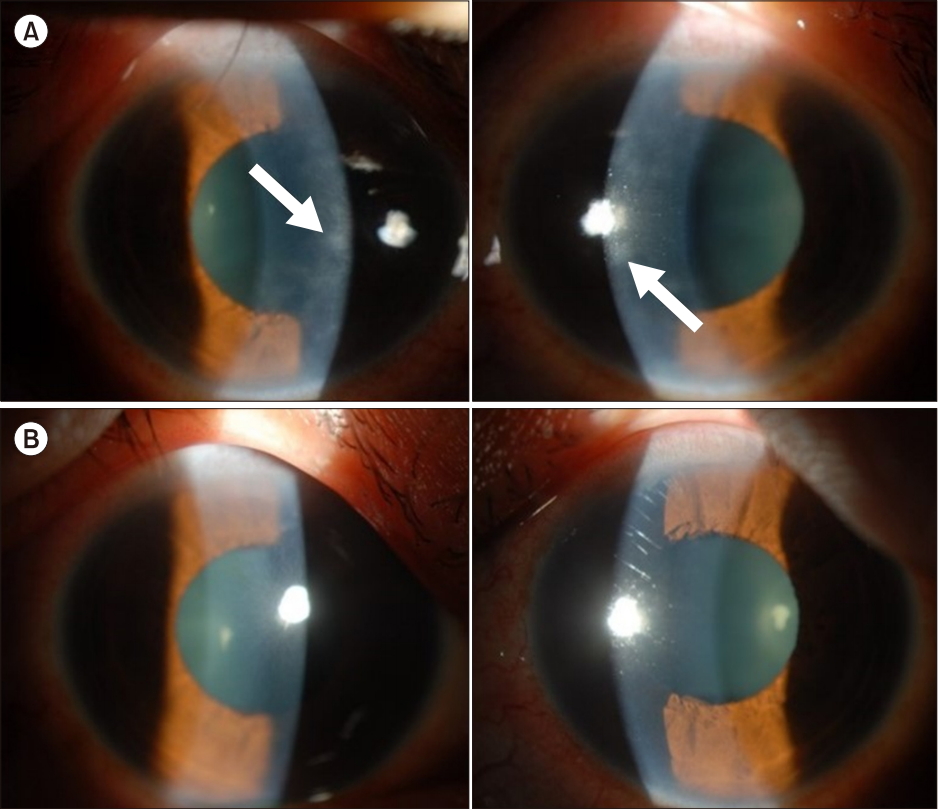
Fig. 4.(A) A slit-lamp examination reveals a stromal infiltration in both eyes at second admission (arrow). (B) After systemic steroid treatment, the stromal infiltration disappeared.
- 1. Cogan DG. Syndrome of nonsyphilitic interstitial keratitis and vestibulo-auditory symptoms. Arch Ophthalmol 1945;33:144–9.Article
- 2. Haynes BF, Kaiser-Kupfer MI, Mason P, Fauci AS. Cogan syndrome: studies in thirteen patients, long-term follow-up, and a review of the literature. Medicine (Baltimore) 1980;59:426–41.ArticlePubMed
- 3. Cheson BD, Bluming AZ, Alroy J. Cogan’s syndrome: a systemic vasculitis. Am J Med 1976;60:549–55.ArticlePubMed
- 4. Iliescu DA, Timaru CM, Batras M, De Simone A, Stefan C. Cogan’s syndrome. Rom J Ophthalmol 2015;59:6–13.PubMedPMC
- 5. Grasland A, Pouchot J, Hachulla E, Blétry O, Papo T, Vinceneux P, et al. Typical and atypical Cogan's syndrome: 32 cases and review of the literature. Rheumatology (Oxford) 2004;43:1007–15.ArticlePubMed
- 6. Seo JD, Choi JH, Choi KD. Multiple cerebral infarction in Cogan's syndrome. Res Vestib Sci 2014;13:85–8.
- 7. Pysden KS, Long V, Ferrie CD, Leeds Teaching Hospitals NHS Trust. Cogan's syndrome: a rare cause of meningoencephalitis. J Child Neurol 2009;24:753–7.ArticlePubMed
- 8. Albayram MS, Wityk R, Yousem DM, Zinreich SJ. The cerebral angiographic findings in Cogan syndrome. AJNR Am J Neuroradiol 2001;22:751–4.PubMedPMC
- 9. Karni A, Sadeh M, Blatt I, Goldhammer Y. Cogan’s syndrome complicated by lacunar brain infarcts. J Neurol Neurosurg Psychiatry 1991;54:169–71.ArticlePubMedPMC
- 10. Ho AC, Roat MI, Venbrux A, Hellmann DB. Cogan's syndrome with refractory abdominal aortitis and mesenteric vasculitis. J Rheumatol 1999;26:1404–7.PubMed
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite




