
Articles
- Page Path
- HOME > Res Vestib Sci > Volume 21(3); 2022 > Article
-
Original Article
전정신경초종 환자에서 어지럼 유무에 따른 전정기능 -
이영정1, 이세아1, 이익성2, 이태경2, 이종대1

- Impairment of Vestibular Function in Patients with Vestibular Schwannoma According to the Presence of Dizziness
-
Youngjeong Lee1, Se A Lee1, Eek-Sung Lee2, Tae-Kyeong Lee2, Jong Dae Lee1
-
Research in Vestibular Science 2022;21(3):75-79.
DOI: https://doi.org/10.21790/rvs.2022.21.3.75
Published online: September 15, 2022
1Department of Otorhinolaryngology-Head and Neck Surgery, Soonchunhyang University Hospital Bucheon, Korea
2Department of Neurology, Soonchunhyang University Hospital Bucheon, Bucheon, Korea
- Corresponding Author: Jong Dae Lee Department of Otorhinolaryngology-Head and Neck Surgery, Soonchunhyang University Hospital Bucheon, 170 Jomaru-ro, Wonmi-gu, Bucheon 14584, Korea Tel: +82-32-621-5015 Fax: +82-32-621-5016 E-mail: ljdent@schmc.ac.kr
Copyright © 2022 by The Korean Balance Society.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,821 Views
- 56 Download
Abstract
-
Objectives:
- Vestibular schwannoma (VS) is a benign Schwann cell-derived slow growing tumor originating from the vestibular nerve. Here, we aimed to investigate the correlation between the presence of the dizziness symptoms and several vestibular function test results.
-
Methods:
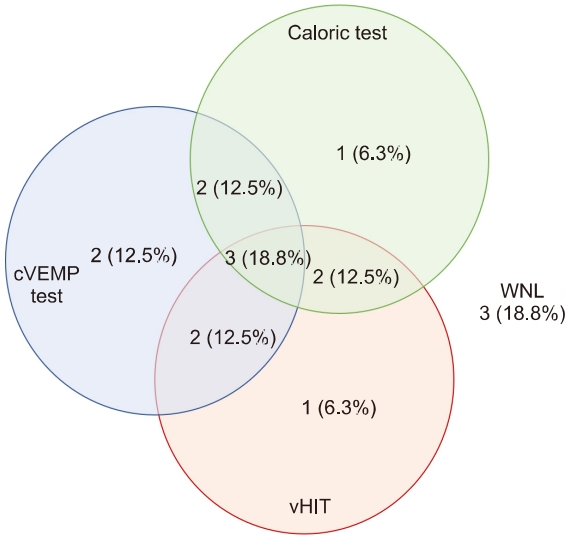
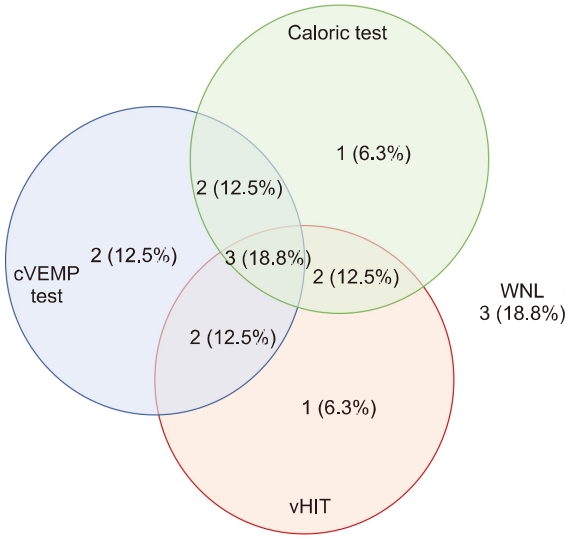
- We analyzed 32 patients who diagnosed with VS from 2010 to 2021 in our hospital. Caloric test, cervical vestibular-evoked myogenic potential (cVEMP) test, and video head impulse test (vHIT) were analyzed.
-
Results:
- Age, sex, pure tone audiometry, and tumor size did not show any statistical significance according to the presence or absence of dizziness. There was also no association between the presence of dizziness symptom or dizziness type and the results of the caloric test, vHIT, and cVEMP test, respectively. However, patients with dizziness had a higher rate of tumors confined to the inner auditory canal than those without dizziness.
-
Conclusions:
- In this study, the rate of complaints of dizziness was higer in patients with intracanalicular VS. The diagnostic role of vestibulsr function tests in VS is limited. The dissociation of the results of caloric test, vHIT, and cVEMP test suggest that these test are complementary.
서 론
대상 및 방법
결 과
고 찰
-
이해관계(CONFLICT OF INTEREST)
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
-
연구 지원(FUNDING/SUPPORT)
이 연구는 순천향대학교 연구 기금의 지원을 받았습니다.
-
저자 기여(AUTHOR CONTRIBUTIONS)
Conceptualization, Funding acquisition, Project administration: JDL; Data curation: YL; Formal analysis: YL, SAL; Investigation: YL; Methodology: YL, SAL, JDL; Visualization: SAL; Writing–original draft: YL, SAL, JDL; Writing–review & editing: all authors.
All authors read and approved the final manuscript.
ARTICLE INFORMATION
| Function | Vertigo (n=5) | Disequilibrium (n=10) | p-value |
|---|---|---|---|
| Abnormal canal paresis (%) | 60.0 | 50.0 | 0.573 |
| Abnormal cVEM P test (%) | 40.0 | 70.0 | 0.287 |
| Abnormal vHIT (%) | 40.0 | 60.0 | 0.427 |
- 1. Møller MN, Hansen S, Caye-Thomasen P. Peripheral vestibular system disease in vestibular schwannomas: a human temporal bone study. Otol Neurotol 2015;36:1547–53.PubMed
- 2. DeLong M, Kirkpatrick J, Cummings T, Adamson DC. Vestibular schwannomas: lessons for the neurosurgeon. Part II: molecular biology and histology. Contemp Neurosurg 2011;33:4.
- 3. Gal TJ, Shinn J, Huang B. Current epidemiology and management trends in acoustic neuroma. Otolaryngol Head Neck Surg 2010;142:677–81.ArticlePubMedPDF
- 4. Chae SW, Kim MG, Choi JH, Hwang SJ. MRI technique for the detection of acoutic neuroma. Korean J Otolaryngol-Head Neck Surg 2000;43:488–92.
- 5. Foley RW, Shirazi S, Maweni RM, Walsh K, McConn Walsh R, et al. Signs and symptoms of acoustic neuroma at initial presentation: an exploratory analysis. Cureus 2017;9:e1846. ArticlePubMedPMC
- 6. Chung WH, Hong SH, Cho YS, Kim SM, Chang BC, Choi JY, et al. Characteristics of vertigo manifestations and vestibular function tests in patients with acoustic neuroma according to the tumor size. Korean J Otolaryngol-Head Neck Surg 2000;43:7–14.
- 7. Andersen JF, Nilsen KS, Vassbotn FS, Møller P, Myrseth E, Lund-Johansen M, et al. Predictors of vertigo in patients with untreated vestibular schwannoma. Otol Neurotol 2015;36:647–52.ArticlePubMed
- 8. Nilsen KS, Lund-Johansen M, Nordahl SH, Finnkirk M, Goplen FK. Long-term effects of conservative management of vestibular schwannoma on dizziness, balance, and caloric function. Otolaryngol Head Neck Surg 2019;161:846–51.ArticlePubMedPDF
- 9. Lee JD, Park MK, Lee BD, Park JY, Lee TK, Sung KB. Otolith function in patients with head trauma. Eur Arch Otorhinolaryngol 2011;268:1427–30.ArticlePubMedPDF
- 10. Fujiwara K, Morita S, Fukuda A, Akamatsu H, Yanagi H, Hoshino K, et al. Analysis of semicircular canal function as evaluated by video Head Impulse Test in patients with vestibular schwannoma. J Vestib Res 2020;30:101–8.ArticlePubMed
- 11. Carlson ML, Link MJ. Vestibular schwannomas. N Engl J Med 2021;384:1335–48.ArticlePubMed
- 12. Carlson ML, Tveiten ØV, Driscoll CL, Goplen FK, Neff BA, Pollock BE, et al. What drives quality of life in patients with sporadic vestibular schwannoma? Laryngoscope 2015;125:1697–702.ArticlePubMed
- 13. Batuecas-Caletrio A, Santa Cruz-Ruiz S, Muñoz-Herrera A, Perez-Fernandez N. The map of dizziness in vestibular schwannoma. Laryngoscope 2015;125:2784–9.ArticlePubMed
- 14. Kjærsgaard JB, Szeremet M, Hougaard DD. Vestibular deficits correlating to Dizziness Handicap Inventory score, hearing loss, and tumor size in a Danish cohort of vestibular schwannoma patients. Otol Neurotol 2019;40:813–9.ArticlePubMed
- 15. Selesnick SH, Jackler RK, Pitts LW. The changing clinical presentation of acoustic tumors in the MRI era. Laryngoscope 1993;103(4 Pt 1):431–6.ArticlePubMed
- 16. Godefroy WP, Hastan D, van der Mey AG. Translabyrinthine surgery for disabling vertigo in vestibular schwannoma patients. Clin Otolaryngol 2007;32:167–72.ArticlePubMed
- 17. Nam SI. Diagnosis and management of vestibular schwannoma: focus on dizziness. Res Vestib Sci 2021;20:119–25.ArticlePDF
- 18. Taylor RL, Kong J, Flanagan S, Pogson J, Croxson G, Pohl D, et al. Prevalence of vestibular dysfunction in patients with vestibular schwannoma using video head-impulses and vestibular-evoked potentials. J Neurol 2015;262:1228–37.ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- We recommend
- Related articles
-
- A Comparative Analysis of the Vestibulocochlear Function in Patients with Isolated Semicircular Canal Hypofunction Using a Video Head Impulse Test
- Diagnosis and Management of Vestibular Schwannoma: Focus on Dizziness
- Customized Vestibular Rehabilitation in the Patients with Bilateral Vestibulopathy: A Pilot Study in One Referred Center
- Customized vestibular rehabilitation in the patients with bilateral vestibulopathy: A pilot study in one referred center
- The Clinical Efficacy of Vestibular Function Tests in Patients with Acute Unilateral Vestibulopathy

