뇌줄기 뇌졸중으로 인한 어지럼증
Vascular Origin of Central Vertigo: Brainstem
Article information

Abstract
Abstracts
Various neurotologic findings can be observed in stroke involving the brainstem. Analyses of the neurotologic findings are important in brainstem stroke since it can have negative diffusion-weighted image, as well as, presenting with acute vestibular syndrome in isolation without any associated neurologic deficits. In this review we discuss the neurotologic findings from lesion involving (1) the medial vestibular nucleus, (2) nucleus prepositus hypoglossi, (3) inferior cerebellar pe-duncle, (4) medial longitudinal fasciculus, (5) rostral interstitial nucleus of the medial longitudinal fasciculus, (6) interstitial nucleus of Cajal, and (7) middle and (8) superior cerebellar peduncles. It is important to recognize these specific neurotologic findings depending on the neural structures involved that may guide early detection and proper management.
서론
갑작스럽게 발생하며 24시간 이상 지속되는 회전성 어지럼증이 주된 증상인 급성 전정 증후군(acute vestibular syndrome)은 대개 전정신경염을 위시한 말초성 전정 병변으로 인해 발생하나, 뇌줄기나 소뇌 같은 후방 순환영역 뇌졸중(posterior circulation stroke)에 의해서도 종종 나타날 수 있어 진단에 주의를 요한다. 실제로, 후방 순환영역 뇌졸중 환자 중 62%는 적어도 한 차례 이상의 급성 어지럼증을 경험하며, 후방 순환영역 뇌졸중 초기증상의 19%는 급성 어지럼증이다[1,2]. 후방 순환영역의 뇌졸중은 국소적 신경학적 이상 없이 급성 어지럼증 단독으로 발현할 수 있으며, 뇌혈관 이상에 의한 어지럼증의 영상학적 진단 정확도는 35%로 매우 낮다[3–6]. 특히 뇌줄기에는 안구운동을 담당하는 뇌신경 및 신경핵들이 밀집해 있어, 뇌줄기를 침범하는 뇌졸중의 경우 각종 안진 및 안구운동 장애가 흔하게 관찰되므로 이를 정확하게 해석하고 진단하는 것이 중요하다[7,8]. 이 종설에서는 뇌줄기의 국소병변으로 인해 나타날 수 있는 신경이과 소견에 대해 정리하고자 한다.
본론
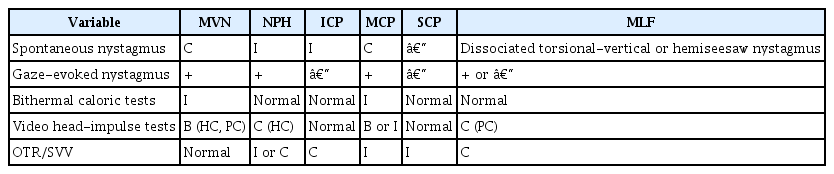
신경구조물에 따른 눈운동 이상을 Table 1에 간략히 정리하였다.
1. 내측전정핵(medial vestibular nucleus)
전정핵은 꼭대기쪽 연수와 바닥쪽 교뇌의 등가측 부위 (dorsolateral portion)에 위치한다(Fig. 1). 내측전정핵은 말초 전정신경의 정보가 교차하는 부위로, 해당 부위가 손상되면 말초성 및 중추성 전정기능 장애가 혼재해 나타나게 된다[7]. 즉 병변 반대편으로의 자발안진, 병측으로의 두부충동검사 양성 소견을 보이거나 온도안진검사에서 반고리관 마비(canal paresis)를 보일 수 있어, 말초신경병증으로 쉽게 오인될 수 있다(pseudo-vestibular neuritis). 하지만 전정신경염과는 달리 비디오 두부충동검사나 자기추적 코일(magnetic search coil)에서 병측 뿐 아니라 건측 수평 및 후반고리관의 전정안반사 이득이 감소된 양상을 보인다. 이는 내측전정핵 손상에 따른 건측으로의 억제성사이신경원(interneuron)도 기능이 저하되며, 이에 대한 적응기제로 양측의 전정안반사 이득이 감소한 것으로 설명한다[9].

Neural substrates respon-sible for eye movements in pons and medulla. HN, hypoglossal nu-cleus; MLF, medial longitudinal fasciculus; LVN, lateral vestibular nucleus; AN, abducens nucleus; MVN, medial vestibular nucleus; ICP, inferior cerebellar peduncle; IVN, inferior vestibular nucleus; NPH, nucleus prepositus hypoglossi.
또한 내측전정핵은 설하전 신경핵과 더불어, 뇌줄기에서 수평면의 신경 적분체(neural integrator)로 기능한다[10]. 가측 주시 시에 안와에 존재하는 인대와 근육에 의한 복원력에 의해 안구에는 다시 정위로 돌아가려는 복원력이 작용하게 된다. 신경 적분체들은 전운동 신경원(premotor neuron)으로부터 전달받은 속도 정보를 적분하여 안구 움직임의 목표 지점의 위치 정보를 안구운동 신경원으로 산출해주는 중개 역할을 하여, 가측 주시 시 안구가 중심으로 끌려가지 않고 목표점에 원하는 만큼 머무를 수 있게 한다. 따라서, 내측전정핵을 포함한 신경 적분체에 병변이 발생하면 수평 주시유발안진(gaze-evoked nystagmus)이 발생하며[11], 이 경우 안진 서상의 파형(waveform)은 대개 특징적으로 감소 서상(decelerating slow-phase velocity)의 양상을 띤다. 안구 기울임 반응 및 주관적 시축 검사는 대개 내측전정핵 병변에서 정상 소견을 보인다[11].
2. 설하전 신경핵(nucleus prepositus hypoglossi)
설하전 신경핵은 내측전정핵, 소뇌 타래엽(flocculus)와 함께 수평 방향의 신경 적분체로 기능하며 교뇌-연수 접합부의 등측 및 내측전정핵의 내측에 위치한다(Fig. 1). 설하전 신경핵은 올리브핵, 소뇌 타래엽을 거쳐 반대편의 내측전정핵에 흥분성 날신경(efferent) 신호를 전달하며, 따라서 이 부위에 병변이 생기면 병변측 소뇌 타래엽 및 반대편 전정핵의 기능이 저하된다[12]. 따라서 설하전 신경핵의 병변은 수평성 주시유발안진 외에 병변측으로의 자발안진 및 건측으로의 두부충동검사 이상을 보이나, 온도안진검사는 정상 소견을 보인다[9,12]. 안구 기울임 반응 및 주관적 시축 비틀림은 병변측이나 병변 반대편으로 비슷한 빈도로 관찰된다[12].
3. 아래소뇌다리(inferior cerebellar peduncle)
뇌줄기와 소뇌는 3개의 소뇌다리를 통해 연결되는데, 아래소뇌다리는 등측 척수소뇌로(dorsal spinocerebellar tract)로서, 올리브핵 및 전정핵으로부터의 소뇌의 날신경 섬유들이 아래소뇌다리를 통해 주행한다[13]. 이 섬유들을 통해 전달되는 고유감각(proprioceptive), 체성 감각 및전정 감각들을 소뇌에서 통합하는데, 아래소뇌다리에 뇌졸중이 발생하면 급성 전정신경병증이 발현할 수 있다. 통상적으로 아래소뇌다리 병변에서 보이는 신경안과적 소견은 병측으로의 자발안진과 체측방돌진(body latero-pulsion), 병변 반대편으로의 주관적 시축 비틀림 및 안구 기울임 반응이 특징적이다[14]. 최근의 연구에서 원지성(apogeotropic) 중추성 체위안진이 발생할 수 있다고 보고하였으며, 이는 소뇌 결정 결절(nodulus)나 전방 목젖(uvula), 편도(tonsil)로의 날신경 섬유들의 침범으로 인해 발생한다고 추측된다(Fig. 2) [15].

Neural connection between the nodulus (N) and vestibular nuclei complex (VN). ICP, inferior cerebellar peduncle.
4. 안쪽세로다발(medial longitudinal fasciculus)
동안신경과 외전신경을 연결해주는 안쪽세로다발에 병변이 생기면 핵사이안근마비(internuclear ophthalmoplegia)가 발생한다. 핵사이안근마비 환자에서 병변측 내전 장애(adduction limitation) 및 병변 반대편 주시 시에 외전안에서 해리성 외전안진(dissociated abducting nystagmus)이 관찰되는 것이 특징적이다[10]. 이러한 해리성 안진이 나타나는 기전은 내직근 마비를 보상하기 위한 신경 발화의 증가가 헤링의 법칙(Hering's law of equal innervation)에 의해 반대편 외직근에도 같이 전달되기 때문으로 생각되어 왔다. 하지만, 최근 연구에 의하면 내직근 마비로 인해 발생하는 외전안의 속도 정보(pulse)와 위치 정보(step) 간의 부조화(pulse-step mismatch)로 인해 해리성 안진이 발생한다고 하였다. 즉, 안구 장애에 대한 적응기제로 정중곁 교뇌 그물체(paramedian pontine reticular formation)의 pulse discharge가 증가하는 데 반해 step signal은 불변함으로써 해리성 안진이 발생하며[16,17], 이러한 연유에서 안진보다는 속진(saccadic intrusion)에 합당한 안구운동 이상으로 간주되기도 한다.
드물게 반시소 안진(hemiseesaw nystagmus)이나, 수직 방향의 해리안진이 관찰되기도 한다. 전자는 양측 눈의 회선성분은 공액성으로 움직이나, 수직성 벡터는 반대 방향의 안진이 관찰되는 경우를 말한다. 후자는 한쪽 눈에서는 수직안진이, 반대편 눈에서는 회선안진이 주로 관찰되는 경우로, 이러한 안진들은 전방 및 후방고리관의 전정안반사로가 선택적으로 침범함으로써 발생하는 것으로 알려져 있다[18,19].
안쪽세로다발 병변에서는 눈기울임반응(ocular tilt re-action)이 흔하게 발생하는데, 이는 중력 감지로(graviceptive pathway)가 안쪽세로다발을 통해 주행하기 때문이다[20,21]. 이에 대해서는 뒤에서 다시 설명하기로 한다.
5. 안쪽세로다발입쪽사이질핵(rostral interstitial nucleus of the medial longitudinal fasciculus)
안쪽세로다발입쪽사이질핵은 중뇌의 위둔덕(superior colliculus) 높이에서 뇌간의 정중선의 내측 및 중뇌 수도관(aqueduct) 배측에 위치한다(Fig. 3). 안쪽세로다발입쪽사이질핵의 병변은 대개 덮개앞증후군(pretectal syndrome)의 일부로 상방 주시 마비가 흔하게 관찰된다[10,22]. 환자들은 신속안구운동이나 원활추종운동 같은 의도적(vol-itional) 안구운동을 통해서는 상방 주시가 불가능한데 반해, 수직 전정안반사에 의해서는 안구 마비가 극복되는 특징적인 핵위마비(supranuclear palsy)의 양상을 보인다. 눈모음(convergence)도 대부분 가능치 않으며, 카할사이핵 병변에서는 동측으로 향하는 회선 자발안진이 보이는 데 반해[23], 안쪽세로다발입쪽사이질핵에서는 반대편으로 향하는 안진이 관찰된다[24].

Neural substrates respon-sible for eye movements in the brainstem. INC, interstitial nucleus of Cajal; MLF, medial longitudinal fasciculus; riMLF, rostral inter-stitial nucleus of the MLF; III, ocu-lomotor nucleus; IV, trochlear nu-cleus; VI, abducens nucleus.
6. 카할사이핵(interstitial nucleus of Cajal)
카할사이핵은 수직면과 회선성 주시 유지에 신경 적분체로서 중요한 역할을 하며 병변이 생길 경우 수직면의 주시유발안진이 발생한다. 뇌졸중은 대부분 카할사이핵의 일측성 기능이상을 유발하는데, 이로 인해 동측으로의 회선안진 및 머리기울임(head tilt) 반응이 유발될 수 있다.
머리기울임 반응이 발생하는 원리는 다음과 같다. 머리를 한쪽으로 기울이면 동측의 타원낭(utricle) 및 전방 및 후방 반고리관이 자극되는데, 이로 인해 동측 안구의 상사근, 상직근, 반대편의 하사근과 하직근을 흥분시켜, 고개를 기울인 쪽의 안구는 내회선 및 상전, 고개를 기울인 반대편의 안구는 외회선 및 하전이 발생하게 된다. 눈기울임 반응은 이러한 중력 감지로의 이상이 생길 경우발생하는데, 이는 전방 및 후방 반고리관과 타원낭에서부터 시작되어 관상 회전면(roll plane)의 전정안반사를 관장하는 동안신경, 활차신경핵을 거쳐 반대편 카할사이핵 및 안쪽세로다발입쪽사이질핵에 다다르는 경로 어디에서건 병변이 생기면 발생할 수 있다[25]. 눈기울임반응은 머리기울임, 스큐편위(skew deviation), 안구회선(ocular torsion)의 3가지 반응으로 이루어지며, 말초 전정 및 하부 뇌간 병변에서는 병변 쪽으로 눈기울임반응이 발생하고, 상부 뇌간 병변에서는 병변 반대편으로 발생한다[26]. 눈기울임반응은 3가지 현상이 모두 관찰될 수도 있으나, 환자에 따라서는 일부만 나타나는 경우도 흔하다.
7. 중간소뇌다리(middle cerebellar peduncle)
중간소뇌다리는 전하소뇌동맥(anterior inferior cerebellar artery)이 혈류를 공급하는데, 미로에 혈류를 공급하는 미로동맥 또한 전하소뇌동맥으로부터 분지되어 총와우동맥(common cochlear artery)과 앞전정동맥(anterior vestibular artery)을 내게 된다[27]. 이러한 이유로 전하소뇌동맥 경색에서는 흔하게 미로도 허혈성 손상을 받게 되며 중간소뇌다리 뇌졸중에서는 급성 청력 저하 외에도 전정의 손상에 따른 말초성 전정병증이 같이 동반한다[28]. 전하소뇌동맥은 소뇌 타래에도 혈류를 공급하는데, 경우에 따라선 소뇌 타래 침범에 따른 중추성 안진과 미로 손상에 의한 말초성 안진이 혼합되어 나타날 수 있어 해석에 주의를 요한다[9,29].
8. 위소뇌다리(superior cerebellar peduncle)
위소뇌다리에는 소뇌로부터 적핵(red nucleus), 시상 및 시상하부, 교뇌 그물체, 올리브핵에 이르는 대부분의 소뇌 들신경섬유(afferent fibers)들이 주행하지만, 배측 척수소뇌로(ventral spinocerebellar fiber)같은 일부 날신경섬유들도 위소뇌다리를 거쳐 뇌줄기 및 대뇌로 향하게 된다. 바닥쪽 소뇌와 달리 꼭대기쪽 소뇌는 안구운동에는 크게 관여하지 않는 것으로 알려져 있어 위소뇌다리 병변에서도 특별한 눈운동이상은 보이지 않으나, 일부 환자에게서 동측으로의 체측방돌진 및 눈기울임반응, 중추성 체위안진을 보일 수 있다고 알려져 있다[30,31].
결론
뇌줄기에는 안구운동을 담당하는 뇌신경이 밀집되어 있어 여러 양상의 눈운동이상 및 안진이 다양하게 나타난다. 뇌줄기에 허혈성 병변이 발생하는 경우 자기공명영상에서 정상을 보이는 경우도 있으며, 다른 신경학적 증상이나 징후 없이 급성 전정 증후군 단독으로 발현할 수 있다. 또한 뇌줄기 병변으로 인해 말초성 및 중추성 안진이 혼합되어 나타날 수 있기 때문에 해석에 유의해야 한다. 따라서 앞에서 열거한 특정 신경학적 구조물 침범에 따른 눈운동의 양상을 이해하는 것이 중추성 어지럼증을 진단하는 데 있어 중요하다 하겠다.
중심 단어: 안진, 중추 현훈, 뇌줄기
이해관계(CONFLICT OF INTEREST)
저자는 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.