반복적인 기립어지럼을 호소한 후하소뇌동맥협착증
Posterior Inferior Cerebellar Artery Stenosis Presenting as Recurrent Orthostatic Dizziness
Article information

Trans Abstract
We report a unique case of vertebrobasilar transient ischemic attacks manifesting as isolated, recurrent, orthostatic dizziness with posterior inferior cerebellar artery (PICA) stenosis. A 57-year-old male patient without past medical history, presented with brief orthostatic dizziness for 2 weeks. There was no associated nausea, vomiting, diplopia, or weakness. On neuro-otologic examination, the patient did not show spontaneous, positional, or gaze-evoked nystagmus. Vestibular function tests such as caloric test, head impulse test, video-oculography, and tilt table test were normal. Brain diffusion-weighted images showed multiple small high signal intensities in the bilateral cerebellar hemispheres. Brain magnetic resonance angiography revealed hypoplasia of the right vertebral artery without focal intracranial focal stenosis. Four-vessel cerebral angiogram showed severe stenosis at the right PICA artery. Our patient’s clinical scenario appears unique hemodynamic spells without symptoms or signs of posterior circulation ischemia. Physicians should also consider cerebrovascular ischemic when the patient suffers repeated orthostatic dizziness that is not explained clinically.
서 론
척추-기저동맥 일과성 뇌허혈발작(vertebro-basilar transient ischemic attack)은 후뇌순환(posterior circulation)의 허혈로 인한 일시적인 증상이다. 후뇌순환의 허혈은 현훈, 두통, 안진, 근력 저하, 이상감각, 의식 저하, 안면마비 등의 다양한 증상이 나타날 수 있다[1]. 후하소뇌동맥(posterior inferior cerebellar artery)에 국한된 뇌경색은 국소적인 신경학적 이상이 없는 단독 어지럼이나 현훈, 균형장애를 호소할 수 있다[2-4]. 저자들은 척추-기저동맥 일과성 뇌허혈발작 증상으로 반복적인 기립성 어지럼을 보인 우측 후하소뇌동맥 협착의 증례를 경험하여 보고하고자 한다.
증 례
기저질환 없는 57세 남자 환자가 2주 전부터 기립 시 발생하는 반복적 어지럼증과 뒷목 통증을 주소로 내원하였다. 증상은 30초에서 2분 이내에 호전되었으며 아찔한 현기증과 양측으로 휘청이는 균형장애를 호소하였다. 기립 즉시 뒷목 통증이 발생하고 수 초 후에 어지럼증이 발생했는데, 누우면 바로 호전되었으며 앉거나 누워있는 자세에서는 증상이 유발되지 않았다. 어지럼 시 오심, 구토, 복시나 두통, 청력 이상 등은 동반되지 않았다.
내원 당시 시행한 신경이과적 진찰에서 특이소견은 관찰되지 않았으며, 체위성 안진 및 현훈도 관찰되지 않았다. 그 외 신경학적 진찰에서 운동신경, 감각신경, 뇌신경 마비나 소뇌실조 등의 이상은 보이지 않았다. 비침습적 박동간 혈압감시기(noninvasive beat-to-beat blood monitoring; Finometer, Finapres Medical Systems BV, Enschede, the Netherlands)로 시행한 기립경사검사(head-up tilt test)에서 기립저혈압(orthostatic hypotension)이나 체위성기립빈맥증후군(postural tachycardia syndrome)은 관찰되지 않았다(Fig. 1). 추가적으로 시행한 비디오안진검사와 비디오두부충동검사에서 이상 소견은 관찰되지 않았다. 24시간 심전도 기록검사, 심초음파와 심전도에서도 정상 소견을 보였다. 하지만 환자는 여전히 기립 시 반복되는 짧은 어지럼증을 호소하였다. 원인이 뚜렷하지 않은 기립성 어지럼을 감별하기 위해 시행한 뇌 자기공명영상의 확산강조영상에서 여러 개의 작은 고강도 신호의 병변이 관찰되었고(Fig. 2A), 현성확산계수(apparent diffusion coefficient)에서 동일한 영역에 저강도 신호를 보였다(Fig. 2B). 뇌 자기공명혈관촬영술(brain magnetic resonance angiography)에서는 우측 척추동맥의 두개 내에 국소 협착 없는 저형성(hypoplasia) 소견을 보였다(Fig. 3A). 추가적으로 시행한 뇌혈관조영술(transfemoral cerebral angiogaphy)에서 우측 척추동맥의 저형성 및 우측 후하소뇌동맥의 심한 국소 협착 소견을 보였다(Fig. 3B). 또한 우측 소뇌 아래쪽과 소뇌 벌레(cerebellar vermis)는 우측 후하소뇌동맥에서만 혈관을 공급받고 있었다. 환자에게 항혈소판제와 고용량 스타틴(statin)을 투여하였고, 발생 빈도는 서서히 감소하여 1주 후부터 더 이상 기립성 어지럼이 관찰되지 않았다. 퇴원 후 4년 동안 증상은 재발하지 않았으며, 2년 후 시행한 뇌혈관조영술에서 여전히 우측 후하소뇌동맥의 국소 협착이 관찰되었으나 이전 뇌혈관조영술과 비교 시 다소 호전되었다(Fig. 3C).
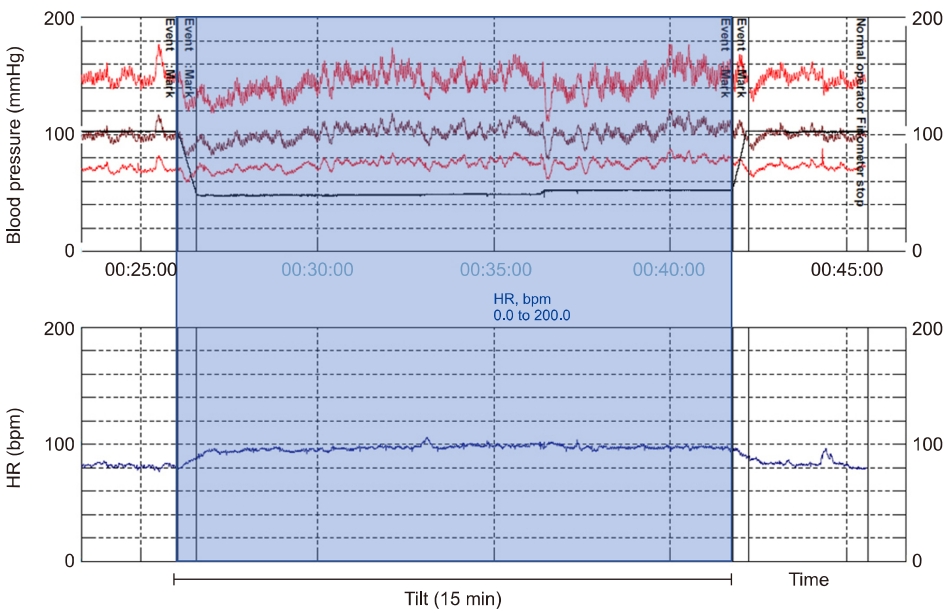
The head-up tilt test showed normal blood pressure and heart rate (HR) responses during autonomic uprising. bpm, beats/min.
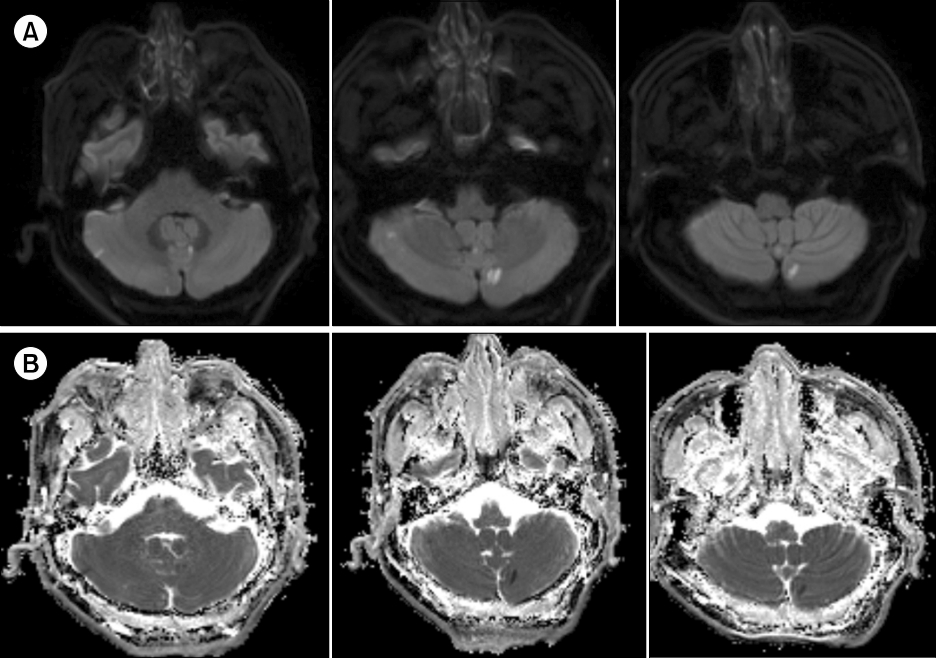
Brain magnetic resonance imaging showed multiple high signal intensities in bilateral cerebellar hemispheres on axial diffusion weight images (A) and low signal intensities on apparent diffusion coefficient (B).
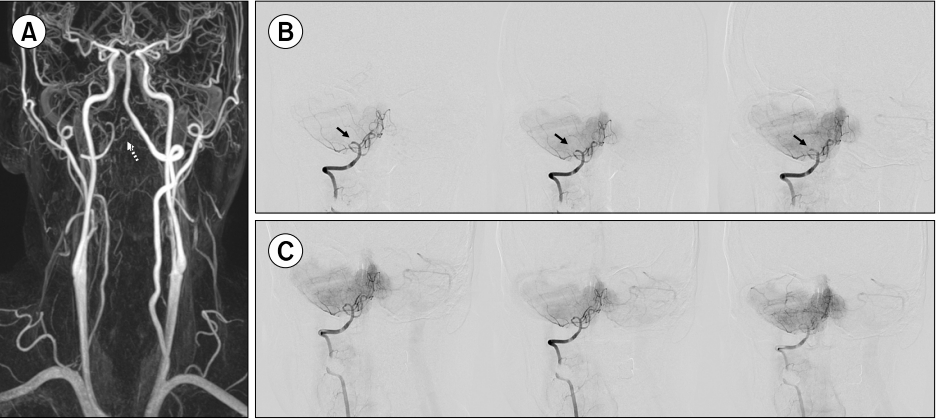
(A) Brain magnetic resonance angiography revealed hypoplasia of the right vertebral artery (dotted arrow). (B) Transfemoral cerebral angiography (TFCA) showed severe stenosis of the right proximal posterior inferior cerebellar artery (PICA) (arrows). (C) Followup TFCA showed also multifocal stenosis of right PICA, but slightly improved compared to the previous study state 2 years ago.
고 찰
기립어지럼은 앉거나 일어설 때, 혹은 서 있거나 걸어다닐 때 발생하고 누우면 호전되는 흔한 어지럼증이다[5]. 기립어지럼은 기립저혈압이나 기립성 빈맥, 실신(syncope), 빈혈(anemia), 심혈관질환 등에 의해 흔하게 발생한다[6,7]. 이러한 질환들은 기립 시 혈류역학(hemodynamic)상 전반적인 뇌혈류량의 감소를 초래하여 어지럼을 유발한다. 일반적으로 현기증으로 나타나지만 30% 가량은 빙빙 도는 양상의 현훈으로 나타나기도 한다[8]. 임상적으로 고립성 실신(isolated syncope)이나 현기증이 있는 환자에서 신경혈관검사를 통해 진단적 도움을 얻는 경우는 매우 낮고[9], 뇌졸중의 위험성을 높이지 않는다[10]. 본 증례와 같이 국소적 신경학적 이상 없이 기립어지럼을 반복적으로 호소하는 척추동맥 저형성을 동반한 후하소뇌동맥 협착 및 뇌경색은 매우 드물다[11]. 본 환자는 저형성된 우측 척추동맥으로부터 소뇌 우측 하부 부위에 혈액을 공급받았고, 후하소뇌경색의 심한 협착으로 인해 반복적인 허혈증상 및 뇌경색이 발생한 것으로 판단된다. 자율신경검사에서 이상소견이 관찰되지 않았으나, 기립은 취약한 혈액 공급을 가중시켰을 것으로 판단되며 동반되는 뒷목 통증과 증상이 길어지는 경우 균형장애도 함께 동반되었다는 것이 임상적인 단서가 될 수 있다.
허혈성 뇌졸중의 20% 정도를 차지하는 후순환(posterior circulation) 허혈은 침범되는 부위에 따라 혼수, 긴신경로 징후(long tract sign), 뇌신경 기능장애 등 다양한 신경학적 이상이 나타날 수 있다[12]. 그러나, 불안정, 비회전성 어지럼, 몸이 좋지 않은 느낌 같은 비국소적 증상도 70% 정도에서 동반되며 경동맥 협착증보다 더 자주 발생한다[13]. 후순환 뇌졸중에 선행하여 발생하는 일과성 전정 증상은 매우 다양하게 나타나는데, 45%에서 자세 변화에 의해 악화되며 55%에서는 수 초 정도 짧은 어지럼을 호소한다[4]. 또한 균형장애를 동반하는 경우는 36%, 현훈을 명확하게 호소하는 경우는 38%였다. 이처럼 후순환 일과성 뇌허혈 증상은 매우 다양하고 비특이적으로 나타날 수 있다.
결론으로, 반복적인 고립성 기립어지럼이 뇌혈관 질환일 가능성이 매우 낮다고 알려져 있으나, 본 증례와 같이 기립어지럼이 두통을 동반하고 척추동맥 저형성 등이 함께 관찰되는 경우 척추뇌기저혈류부전(vertebrobasilar insufficiency)도 의심해보아야 한다. 또한 컴퓨터단층촬영 뇌혈관조영술이나 뇌 자기공명영상 혈관조영술로 뚜렷한 협착 소견을 찾지 못할 경우, 뇌혈관조영술(conventional cerebral angiography)이나 관류 자기공명영상(perfusion magnetic resonance imaging) 등 추가적인 검사를 신속하게 고려해야 하며 취약한 혈액 공급 부위를 확인해야 한다. 척추뇌기저혈류부전이 의심되는 경우 지체 없이 효과적인 치료법을 시행해야 한다.
Notes
이해관계(CONFLICT OF INTEREST)
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
연구 지원(FUNDING/SUPPORT)
해당 없음.
저자 기여(AUTHOR CONTRIBUTIONS)
Conceptualization, Project administration: SJ, JL, JYP; Data curation: SJ, SH; Formal analysis, Methodology: SJ; Investigation: JYP; Visualization: JL, JYP; Writing–original draft: SJJ, JL, JYP; Writing–review & editing: all authors.
All authors read and approved the final manuscript.