고개 회전 시 특징적인 안진을 보이는 척추동맥압박증후군 1예
A Case of Vertebral Artery Compression Syndrome Showing Characteristic Nystagmus during Head Rotation
Article information

A 71-year-old man visited the clinic with a complaint of vertigo that had persisted since the past 2 months. The patient reported that upon turning his head to the left or tilting it backwards, he experienced vertigo, which persisted and worsened until the head was brought back to the straight position. He further complained of tinnitus on the right side that persisted since the development of dizziness. He had undergone brain magnetic resonance imaging (MRI)+magnetic resonance angiography+diffusion to evaluate the tinnitus in his right ear at the neurosurgery department 3 years ago. In these scans, hypoplasia of the right vertebral artery was observed. The examination of nystagmus using Video-Frenzel glasses (SLMED Co., Seoul, Korea) revealed that when the head was turned to the right in the sitting position, there was no dizziness and nystagmus, and upon turning the head to the left, rotational vertigo and left torsional and downward nystagmus were observed. In the Dix-Hallpike position test, there was no nystagmus on the right side, whereas the same nystagmus and dizziness were induced on the left side upon turning the head to the left in the sitting position (Supplementary Video 1 ). He further complained that tinnitus on the right side aggravated when the head was turned to the left, which caused vertigo and nystagmus. In the supine roll test, nystagmus was not induced on either sides.
Cervical spine MRI revealed multiple bony spurs, diffuse posterior bulging discs, and degenerative changes in the C3–T1 spinal segments (Fig. 1). Vertebral artery compression syndrome was confirmed by the observation of compression of the left vertebral artery by the bony spur of the cervical vertebra (C5–6 level) and the rapid decrease of the cerebral blood flow when the head was turned to the left on dynamic four-vessel angiography (Fig. 2). When the head was turned to the left, the basilar artery flow decreased but was maintained. Based on the nystagmus pattern (mixed downbeat, torsional, and horizontal) and accompanying tinnitus in the rotated head position, the vertigo and nystagmus in vertebral artery compression syndrome may be resulted from transient ischemia in the peripheral labyrinth. However, the prominent downbeat nystagmus can be also explained by transient ischemia of the inferior cerebellum. Written informed consent was obtained for publication of this case report and accompanying images.
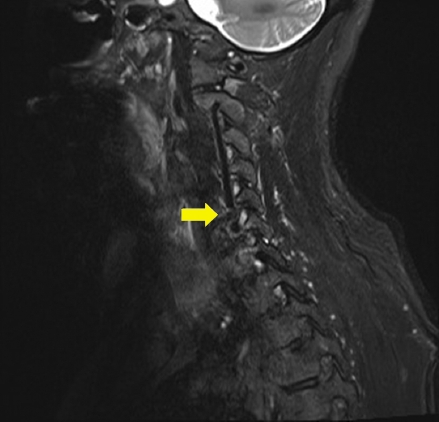
Cervical spine magnetic resonance imaging revealed the protrusion of a bony spur (arrow) that compressed the course of the left vertebral artery.
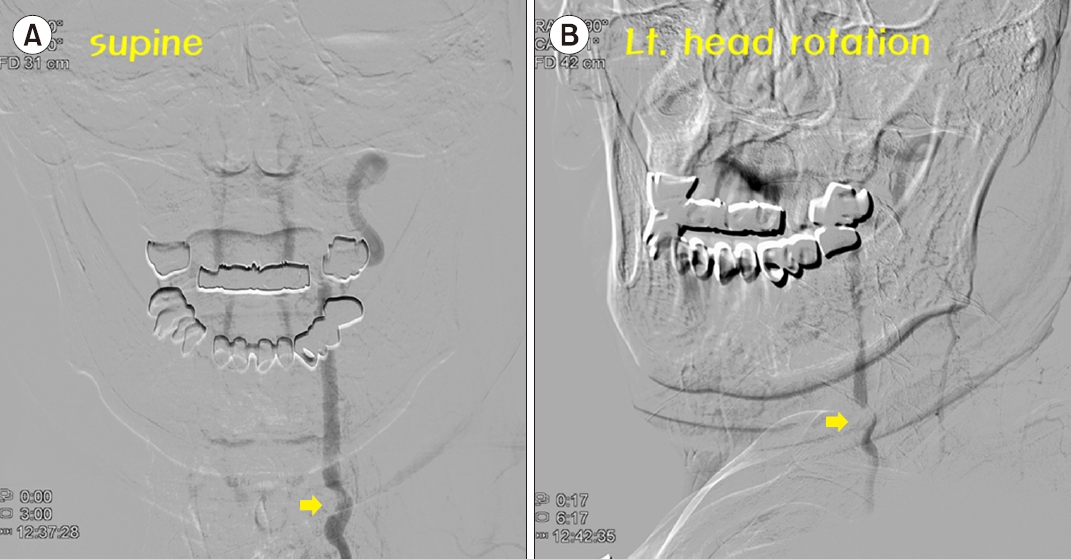
Dynamic four-vessel angiography. (A) Compression of the left vertebral artery by the bony spur (arrow) of the cervical vertebra and (B) rapid decrease in the cerebral blood flow when the head was turned to the left (arrow).
This report was approved by the Institutional Review Board of Incheon St. Mary’s Hospital (No. OC22ZASI0141).
Supplementary materials
Supplementary materials can be found via https://doi.org/10. 21790/rvs.2022.21.4.111.
Video-Frenzel glass examination revealed left torsional and downbeat nystagmus that was induced upon head rotation in the sitting position, which is characteristic of the vertebral artery compression syndrome.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING/SUPPORT
None.